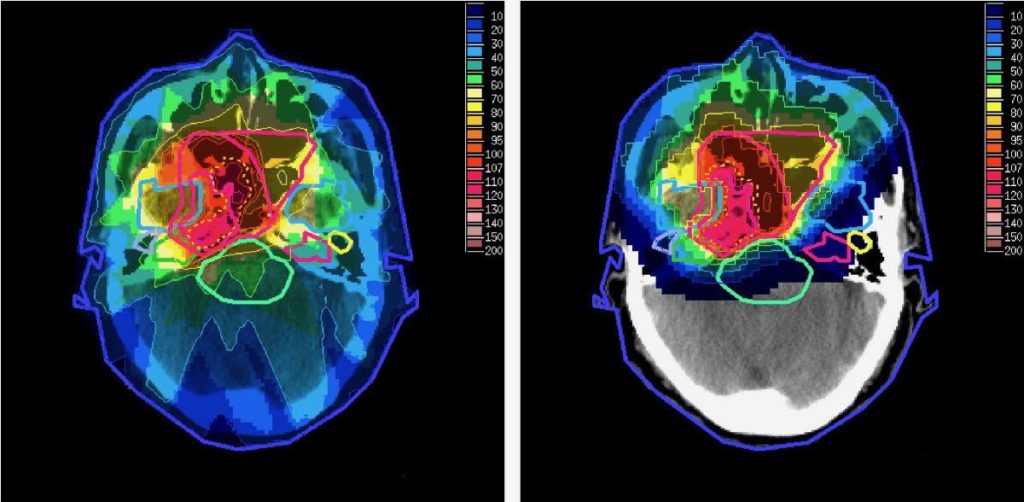
Source: Taheri-Kadkhoda et al. Radiation Oncology 2008 3:4 doi:10.1186/1748-717X-3-4 CC BY 2.0view terms
Stephen McMahon, Queen’s University Belfast
High energy proton beam therapy, an advanced form of radiotherapy, made its debut in the UK in 2018. Both the NHS and private clinics in the U.K. began offering this treatment in the same year, but they treated very different patient groups.
While the NHS used the therapy to treat childhood cancer, private clinics began treating men with prostate cancer.
The situation is similar in other countries. Prostate cancer patients are the most common referral for proton beam therapy in the US and internationally make up the majority treated at many proton centres.
But who sees the greatest benefit from proton beam therapy? And do these benefits justify the substantial cost of treatment (often tens of thousands of pounds)? While there is strong evidence for the benefits of proton therapy in children, it is much less clear in prostate and other adult cancers.
This apparent disconnect between evidence and practice underpins fundamental disagreements about the standard of evidence needed for new treatments and the role of patient choice in healthcare.
Why protons?
Proton therapy is an alternative form of radiotherapy, which is conventionally delivered using X-rays. Both approaches aim beams of radiation at the tumour, killing cancerous cells when they interact with and damage the patient’s DNA. But radiation can also damage healthy tissues and organs that surround the tumour, which can cause side effects.
Modern X-ray radiotherapy minimises these side effects using clever delivery methods. The tumour is treated from many different directions, meaning it can be given a greater dose of radiation while reducing the dose to healthy tissues, and hence the damage. But X-ray radiotherapy still delivers a significant radiation dose to healthy tissues that lie in front of and behind the tumour.
Unlike photons (used in X-ray radiotherapy) which travel right through the body, protons only travel a certain distance through the body before stopping. By carefully tuning this range, it is possible for proton therapy to deliver almost no dose beyond the tumour. This greatly reduces the total dose to healthy tissues.
It is argued that this advantage makes proton therapy a better approach than conventional radiotherapy. And this is true for some cancers. For example, reducing the total dose received by children significantly reduces risks of delays in their development and additional cancers later in life. Protons can also make it easier to deliver precise treatments to tumours close to sensitive organs, such as the spinal cord or optic nerve.
Protons in prostate cancer
In prostate cancer (and many other adult cancers) the benefits are less clear. A big advantage of protons is the reduction in the total dose delivered to the patient. However, the main side effects associated with this are much less significant in adults: delays in development are not a factor, and the risk of additional cancers are much lower as they typically take decades to develop.
Instead, the main side effects are seen in organs close to the prostate that also receive a high dose, such as the bladder and rectum. A high dose must be delivered to a region that includes the prostate and some additional healthy tissues, to make sure the disease is treated fully.
The extra margin allows for the variation that occurs during treatment, such as differences in the way the patient lies down, to make sure the cancer gets a full dose each day. As these patient variations are independent of the radiation type, protons and X-rays typically deliver similar high doses to these healthy tissues.
Despite this, proton therapy has been widely adopted because it is argued the physical benefits are clear, even if small, and will become apparent with time as more people reach the five and ten-year survival mark.
But the results of studies investigating the effects of proton therapy on prostate cancer are mixed. While protons have been shown to an effective treatment for prostate cancer, no consistent advantage has been seen for either long-term survival or quality of life.
One challenge in measuring the benefit of proton therapy for prostate cancer is that conventional radiotherapy is already highly effective. In early stage prostate cancer (stages one to three), nine out of ten men treated with X-rays are expected to remain cancer free after five years.
They also have relatively low rates of long-term side effects compared with many other cancers. As a result, there is a limited scope for proton therapy to improve outcomes, precisely because the outcomes are already so good.
As technology develops this will further reduce side effects and improve rates of remission in conventional radiotherapy, and mean it is increasingly hard to show a benefit from proton beam therapy.
As a result, the NHS and the American Society for Radiation Oncology (ASTRO) do not recommend proton therapy for prostate cancer except as part of a clinical trial. Several of these large international trials are underway, but it will be about a decade before we have conclusive results. Even then, it is expected that protons will represent, at best, an evolution rather than a revolution in prostate cancer radiotherapy.
This has not prevented a demand for prostate proton therapy driving a dramatic expansion in the number of proton therapy centres internationally. In part this is because prostate cancer is one of the most common types of cancer. Treatment for common cancers may actually serve to support the availability of proton therapy for other, rarer cancers. But, it is crucial the benefits for every individual are properly considered.
It is difficult for dry position statements from organisations like the NHS and ASTRO to compete with the dramatic promises proton therapy clinics make. But a balanced discussion of the benefits and costs of all types of radiotherapy is essential to ensure patients have all the evidence to hand before they part with their cash.
Stephen McMahon, Queen’s University Research Fellow, Queen’s University Belfast
This article is republished from The Conversation under a Creative Commons license. Read the original article.