By Fred Schulte, Elizabeth Lucas, Jordan Rau, Liz Szabo, and Jay Hancock, Kaiser Health News
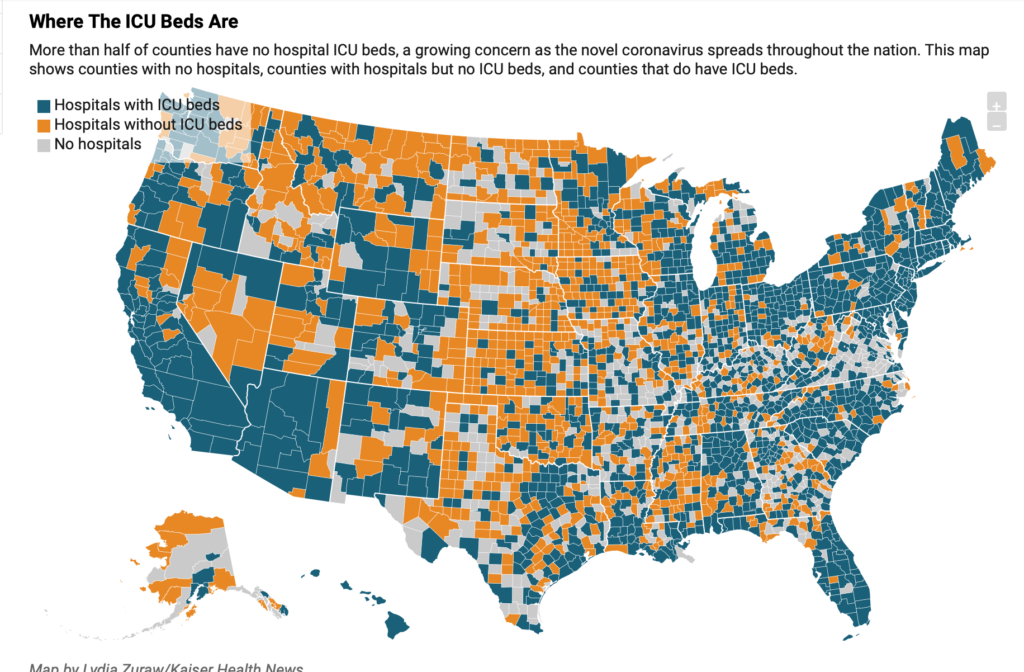
More than half the counties in America have no intensive care beds, posing a particular danger for more than 7 million people who are age 60 and up ― older patients who face the highest risk of serious illness or death from the rapid spread of COVID-19, a Kaiser Health News data analysis shows.
Intensive care units have sophisticated equipment, such as bedside machines to monitor a patient’s heart rate and ventilators to help them breathe. Even in communities with ICU beds, the numbers vary wildly ― with some having just one bed available for thousands of senior residents, according to the analysis based on a review of data hospitals report each year to the federal government.
Consider the homes of two midsize cities: The Louisville area of Jefferson County, Kentucky, for instance, has one ICU bed for every 442 people age 60 or older, while in Santa Cruz, California, that number stands at one bed for every 2,601 residents.
Differences are vast within each state as well: San Francisco, with one bed for every 532 older residents, and Los Angeles, with 847 residents per bed, both have greater bed availability than does Santa Cruz.
Even counties that rank in the top 10% for ICU bed count still have as many as 450 older people potentially competing for each bed.
The KHN findings put in stark relief a wrenching challenge hospitals in many communities — both urban and rural ― could face during the coronavirus pandemic: deciding how to ration scarce resources.
“This is just another example of geography determining access to health care,” Arthur Caplan, a bioethics professor at NYU Langone Medical Center, said when told of KHN’s findings.
Overall, 18 million people live in counties that have hospitals but no ICU, about a quarter of them 60 or older, the analysis shows. Nearly 11 million more Americans reside in counties with no hospital, some 2.7 million of them seniors.
Dr. Karen Joynt Maddox, a professor at Washington University School of Medicine in St. Louis, said that hospitals with larger numbers of ICU beds tend to cluster in higher-income areas where many patients have private health insurance.
“Hospital beds and ICU beds have cropped up where the economics can support them,” she said. “We lack capacity everywhere, but there are pretty big differences in terms of per capita resources.”
Doctors in rural counties are bracing for the possibility they may run out of critical care beds. Northern Light Sebasticook Valley Hospital, in central Maine, has one ventilator and 25 beds. Two of those are “special care” beds that don’t meet full requirements for intensive care but are reserved for the sickest people. Such patients are often transferred elsewhere, perhaps to the city of Bangor, by ambulance or helicopter.
But that may not be possible if COVID-19 surges across the state “because they’re going to be hit just as hard if not harder than we will be,” said Dr. Robert Schlager, chief medical officer at the hospital in rural Pittsfield. “Just like the nation, we probably don’t have enough, but we’re doing the best we can.”
Hospitals also say they can quickly devise plans to transfer cases they can’t handle to other facilities, though some patients may be too ill to risk the move.
Certainly, being in a county with few or no ICU beds may not be as dire as it seems if that county abuts another county with a more robust supply of such beds.
In Michigan, health planners have determined that rural counties with few ICU beds, such as Livingston and Ionia, in the central part of the state, would be served by major facilities in nearby Lansing or Detroit in a major crisis.
Dr. Peter Graham, executive medical director for Physicians Health Plan in Michigan, is affiliated with Sparrow Health System in Lansing. He is making no assumptions. It’s possible central Michigan could take overflow COVID-19 patients from Detroit if that’s where the disease clusters, he said. Or patients might have to be transferred hundreds of miles away.
“It’s just obvious people are going to need to move” if local facilities are overwhelmed, he said. “If we’re able to find a ventilator bed in Indianapolis, in Chicago or Minneapolis or wherever, it is go, get them there!”
Yet experts warn that even areas comparatively rich in ICU beds could be overwhelmed with patients struggling to breathe, a common symptom of seriously ill COVID-19 patients.
“No matter how you look at it, the numbers [of ICU beds] are too small,” said Dr. Atul Grover, executive vice president of the Association of American Medical Colleges. “It’s scary.”
Lenard Kaye, director of the University of Maine Center on Aging, a state with a large older population and relatively few ICU beds, agreed. “The implications are tremendous and very troubling,” he said. “Individuals are going to reach out for help in an emergency, and those beds may well not be available.”
Health workers might need to resort to “triaging and tough decisions,” Kaye said, “on who beds are allocated to.”
That concern isn’t lost on Linnea Olsen, 60, who has lung cancer and knows she is especially vulnerable to any respiratory virus.
Olsen worries about a potential shortage of ventilators and ICU beds, which could lead doctors to ration critical care. Given her fragile health, she fears she wouldn’t make the cut.
“I’m worried that cancer patients will be a low priority,” said Olsen, a mother of three adult children, who lives in Amesbury, Massachusetts.
Olsen, who was diagnosed with lung cancer almost 15 years ago, has survived far longer than most people with the disease. She is now being treated with an experimental medication — which has never been tested before in humans ― in an early-stage clinical trial. It’s her fourth early clinical trial.
“I’m no longer young, but I still would argue that my life is worthwhile, and my three kids certainly want to keep me around,” she said.
She said she has “fought like hell to stay alive” and worries she won’t be given a fighting chance to survive COVID-19.
“Those of us with lung cancer are among the most vulnerable,” Olsen said, “but instead of being viewed as someone to be protected, we will be viewed as expendable. A lost cause.”
Overall, 26 million people live in counties with hospitals but no ICU, about a quarter of them older than 60. Nearly 11 million more Americans reside in counties with no hospital, some 2.7 million of them seniors.
The total number of ICU beds nationally varies, depending on which source is consulted and which beds are counted. Hospitals reported 75,000 ICU beds in their most recent annual financial reports to the government, but that excludes Veterans Affairs’ facilities.
The United States has about three times as many ICU beds per capita as Italy and 10 times as many as China, two countries ravaged by COVID-19, according to a new report from the Society of Critical Care Medicine. The supply of ventilators also exceeds other developed countries, another study found. But as with ICU beds, “there is wide variation [in ventilators available] across states,” the study found.
Many experts predict that demand may soon exceed the supply. Over a period of months, the country may need 1.9 million ICU beds — 20 times the current supply ― to treat COVID-19 patients, according to the American Hospital Association.
Dr. Tia Powell, who co-chaired a 2007 New York State Department of Health group that set guidelines for rationing scarce ventilators, said preventing wildfire-like spread of disease is critical to keeping sick patients from overcrowding hospitals.
“If it spreads slowly, you’re much less likely to run short of critical supplies,” she said. “If you need all of your ventilators right now, this week, that’s what makes trouble.”
Even slowing the pandemic does not guarantee hospitals can cope. While some hospitals are planning to treat patients with less serious illness in tents, it’s far more difficult to create intensive care units or even expand existing ones, said Dr. Greg Martin, president-elect of the Society of Critical Care Medicine, which represents intensive care doctors.
Martin said ventilators need to be hooked up to oxygen and gas lines to supply the appropriate mix of air patients need. To convert a standard hospital unit to an ICU, “you would literally need to tear down the wall and run the piping in,” he said.
Few areas — such as operating rooms, emergency department and units used for post-anesthesia care ― have the hookups needed, according to Martin.
Intensive care units also require specially trained doctors, nurses and respiratory therapists. While nurses in other areas of the hospital may care for six patients, ICU nurses typically focus on one or two, Martin said.
“Mechanical ventilation of a fragile patient is rather dangerous if provided by someone other than these trained ICU professionals, which is why mechanical ventilation is not typically done outside of the ICU,” the group said.
Bob Atlas, president and CEO of the Maryland Hospital Association, noted that hospitals and government officials have been discussing ways to boost staffing levels, such as calling on doctors with expired medical licenses, or those licensed to practice in other states, to treat patients in viral hot spots.
Also up for discussion: loosening rules for “scope of practice,” regulations that spell out the duties medical professionals are permitted based on their training.
Atlas and others said they hope steps hospitals have taken to free up beds, such as deferring nonessential surgery, will keep the system from collapsing.
“It’s not as if every Medicare beneficiary will need an ICU bed,” he said. He also said hospitals could wind up treating only the sickest patients.
Greg Burel, the former director of the Strategic National Stockpile, said he hoped that hospitals lacking ICU beds could quickly iron out transfer agreements to move critically ill patients.
“Let’s hope we don’t get there,” he said.
Novant Health Brunswick Medical Center, on North Carolina’s coast, ordered additional ventilators two months ago in case COVID-19 went global. It has six and expects four more, said Shelbourn Stevens, its president. But it has only five intensive care beds among its 74-bed total.
Drawing on decades of experience with emergency care after hurricanes, the hospital’s staff is decreasing elective-surgery cases and preparing to rapidly increase screening for the new coronavirus.
“I’m very comfortable with our plans right now,” Stevens said. “Disaster planning is in our bones, so to speak. Our team knows how to react.”
But the hospital’s critical-care capacity is limited. North Carolina’s Brunswick County, where it is located, has one bed for every 2,436 residents 60 and older. Such a population could overwhelm the facility in a COVID-19 surge.
If necessary, patients could be transferred to the larger New Hanover Regional Medical Center, a short helicopter ride away, in Wilmington, North Carolina, Stevens said. But with 57 intensive care beds, New Hanover County, which includes Wilmington, still ranks in the lower two-thirds of counties for ICU beds per senior residents.
If the pandemic becomes severe, no amount of critical-care beds will be enough, experts say.
“I liken it to sitting on a Gulf shore when a hurricane is offshore,” said Dr. Graham, from Michigan. “It’s a question of how soon and how hard.”
KHN senior correspondent JoNel Aleccia contributed to this report.
METHODOLOGY
Kaiser Health News evaluated the capacity of intensive care unit (ICU) beds around the nation by first identifying the number of ICU beds each hospital reported in its most recent financial cost report, filed annually to the Centers for Medicare & Medicaid Services. KHN included beds reported in the categories of intensive care unit, surgical intensive care unit, coronary care unit and burn intensive care unit.
KHN then totaled the ICU beds per county and matched the data with county population figures from the Census Bureau’s American Community Survey. KHN focused on the number of people 60 and older in each county because older people are considered the most likely group to require hospitalization, given their increased frailty and existing health conditions compared with younger people.For each county, KHN calculated the number of people 60 and older for each ICU bed. KHN also calculated the percentage of county population who were 60 or older.
KHN’s ICU bed tally does not include Veterans Affairs hospitals, which are sure to play a role in treating coronavirus victims, because VA hospitals do not file cost reports.
The total number of the nation’s ICU beds in the cost reports is less than the number identified by the American Hospital Association’s annual survey of hospital beds, which is the other authoritative resource on hospital characteristics.
Experts attributed the discrepancies to different definitions of what qualifies as an ICU bed and other factors, and told KHN both sources were equally credible.