By Phil Galewitz, KHN
For years, Ely Bair dealt with migraine headaches, jaw pain and high blood pressure, until a dentist recommended surgery to realign his jaw to get to the root of his health problems.
The fix would involve two surgeries over a couple of years and wearing braces on his teeth before and in between the procedures.
Bair had the first surgery, on his upper jaw, in 2018 at Swedish Medical Center, First Hill Campus in Seattle. The surgery was covered by his Premera Blue Cross plan, and Bair’s out-of-pocket hospital expense was $3,000.
He changed jobs in 2019 but still had Premera health insurance. In 2020, he had the planned surgery on his lower jaw at the same hospital where he’d been treated the first time. The surgery went well, and he spent one night in the hospital before being discharged. He was healing well and beginning to see the benefits of the surgeries.
Then the bill arrived.
The Patient: Ely Bair, 35, a quality assurance analyst. He has a Premera Blue Cross health plan through his job at a biotech firm in Seattle.
Total Bill: Swedish Medical Center billed Bair $27,119 for the second surgery in July 2020. This was Bair’s share of the negotiated rate, after the hospital took $14,310 off the charge. His insurer paid $5,000. Bair owed additional bills to the surgeon and the anesthesiologist.
Service Provider: Swedish First Hill Campus in Seattle, part of the largest nonprofit health system in the Seattle area, which is affiliated with Providence, a major Catholic health care network.
What Gives: Bair hit two maddening health system pitfalls here: He expected his new plan to behave like his previous one from the same insurer — and he expected his mouth to be treated like the rest of his body. Neither commonsense notion appears true in America’s health system.
Typically, large companies, such as Bair’s employers, “self insure,” meaning they pay their workers’ health costs but use insurance companies to maintain provider networks and handle claims. When Bair changed jobs, his insurance coverage changed even though both employers used Premera. Bair paid $3,000 for his first surgery because that was the out-of-pocket maximum under his plan from his previous employer, which covered oral and maxillofacial surgery.
Bair’s doctor told him the hospital charge was at least three times the amount Swedish charges uninsured patients for the same surgery. Bair said Swedish offered to let him pay the bill over two years but did not make any other concessions.
Bair expected that using the same hospital and the same insurance carrier would mean his costs would be similar for part two of his treatment. Bair’s oral and maxillofacial surgeon — the same doctor who performed the first procedure — checked Bair’s benefits through his insurer’s online portal and thought it would be covered. Premera also sent his doctor confirmation agreeing that the second procedure was medically necessary.
About three months after the surgery, Bair was shocked to get the large hospital bill — about $24,000 higher than he expected.
When he called Premera, he learned his new plan had a $5,000 lifetime limit on coverage for the reconstructive jaw procedure known as orthognathic surgery, which is sometimes regarded as a dental rather than a medical intervention. His doctor said that information was not noted in Bair’s benefits when the practice reviewed them through an online portal. Premera told Bair he should have known about the limit because it was listed in his detailed, hard-copy, 86-page member-benefit booklet.
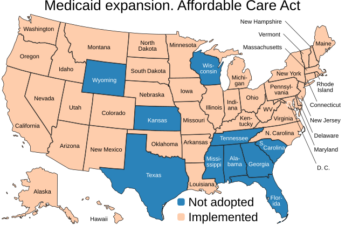
The Affordable Care Act in 2014 eliminated lifetime and annual caps on insurance coverage for categories of treatment such as prescription drugs, laboratory services and mental health care. While the ACA lists broad categories about what is considered an “essential health benefit,” each state decides which services are included in each category and the scope or duration that must be offered. Bariatric surgery, physical therapy and abortion are examples of care for which insurance coverage can vary a lot by state under this ACA provision. Orthognathic surgery is not considered an essential health benefit in Washington. It is sometimes performed for cosmetic purposes only. Also, plans sometimes regard the surgery as part of orthodontia — which frequently involves limits on coverage. But for Bair, it was a clear medical necessity.
Without an ACA requirement for orthognathic surgery, Premera and self-insured plans are allowed to provide various levels of benefits and can impose annual and lifetime caps.
Premera spokesperson Courtney Wallace said Bair transferred from a plan with his former company that did not have a lifetime maximum to a plan with a $5,000 lifetime maximum benefit.
Martine Brousse, a patient advocate and owner of AdvimedPro, which helps patients with health care billing disputes, said Bair acted appropriately by using a doctor and hospital in his health plan’s network and checking with his doctor about his insurance coverage.
She said Swedish should have told him before the surgery — which was planned weeks ahead of time — how much he would have to pay. “That is a failure on part of the hospital,” she said.
Sabrina Corlette, co-director of the Georgetown University Center on Health Insurance Reforms, said it doesn’t seem fair that his first employer covered the cost of his surgery but the second employer did not. She said the $27,000 bill seemed excessive and the $5,000 lifetime limit very low. “Essential health benefits serve a really important function, and when there are gaps or holes people can really get hurt,” she said.
Resolution: Bair’s doctor told him the hospital charge was at least three times the amount Swedish charges uninsured patients for the same surgery. Bair said Swedish offered to let him pay the bill over two years but did not make any other concessions.
Swedish would not say why it did not verify Bair’s insurance benefits before the surgery or let him know he would face an enormous bill even though he was insured.
“Hospital pricing is complex and nuanced,” Swedish officials said in a statement. Bair’s bill “was inclusive of all the care he received, which included specialized services and expertise, equipment and the operating room time. He had a jaw procedure that had a maximum benefit from his insurer of $5,000. He was billed the balance not covered by his insurer.”
The hospital system said it also has an online tool that generates estimates tailored to patients’ coverage and choice of hospital.
The online tool did not come up with anything on the term “orthognathic surgery,” however.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.