
Scott Hagan, University of Washington
Amid the buzz around weight loss drugs and rising rates of obesity worldwide, many health care professionals are questioning one of the key measures that has long been used to define obesity.
On June 14, 2023, the American Medical Association adopted a new policy, calling on doctors to deemphasize the role of body mass index, or BMI, in clinical practice.
The statement by the AMA, the nation’s largest association representing physicians, signals a significant shift in how clinicians regard BMI as a measure of general health. With over 40% of Americans having obesity as defined by BMI, a movement away from BMI could have broad implications for patient care.
As a board-certified obesity medicine physician with a research interest in patient-centered obesity care, I have written before about my concerns over use of BMI as a measure of health. The AMA’s policy statement creates an important opportunity to review the current use of BMI in health care settings and to consider what the future holds for the assessment of the health risks of elevated body weight.
BMI basics
Body mass index is a measurement taken by dividing body weight in kilograms by height in meters squared. The metric was developed to estimate a normal body weight depending on an individual’s height, given that taller people tend to weigh more.
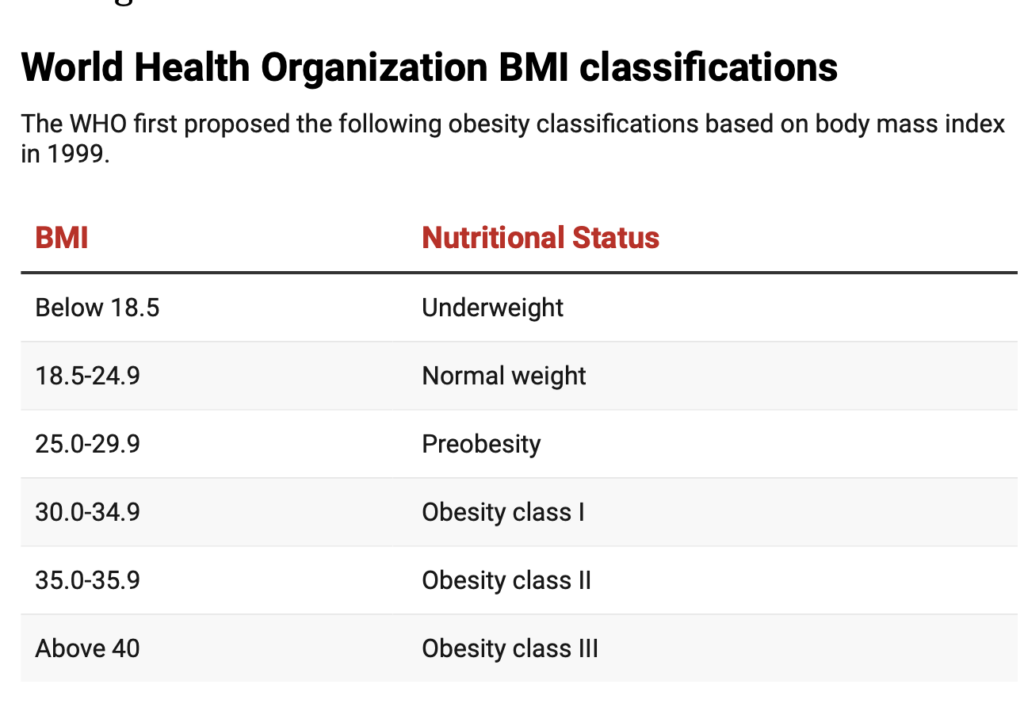
It rose to prominence for clinicians in the 1990s following the World Health Organization’s adoption of the metric as the official screening index for obesity.
Research has consistently shown that BMI at a population level correlates strongly with body fat percentage and risk for serious health conditions. The index is easy to measure and inexpensive to calculate, allowing its wide implementation in health care settings.
Major limitations
Because of that ample body of evidence from previous decades, one of the long-standing assumptions in the use of BMI as a measure of general health is that it accurately predicts an individual’s body fat percentage and, therefore, the potential health risks of elevated weight.
However, while BMI may have strong correlations with the amount of body weight composed of body fat in studies of averages of large groups of people, it does not directly measure body fat for an individual.
Therefore, people with the same BMI may have substantially different body fat percentage based on a variety of factors such as age, muscle mass, sex and race. In an example from one large study, adults with a BMI of 25 had a body fat percentage ranging from 14% to 35% for men, and 26% to 42% for women.
Ultimately, BMI cannot provide doctors with precise information about the portion of body weight composed of body fat, nor can it tell us how that fat is distributed in the body. But this distribution is important because research has shown that fat stored around the internal organs has significantly higher health risks than that distributed in the extremities. https://www.youtube.com/embed/z_3S2_41_FE?wmode=transparent&start=0 You can’t tell if someone is healthy just by looking at their body weight, and using BMI alone to determine if someone is healthy can be misleading.
Further, just as a variety of health factors may affect the accuracy of BMI to predict how much body fat someone has, health outcomes such as developing diabetes at a specific BMI can vary substantially based on factors such as a person’s race, sex, age and physical fitness level.
Finally, a significant number of adults may have metabolically healthy obesity, defined as having a BMI above 30 without having high blood pressure, blood sugar or cholesterol. Adults with metabolically healthy obesity have significantly lower health risks associated with a high BMI and therefore may not benefit from weight loss.
Although research in the 1970s suggested that any BMI above a normal (18.5-24.9) range shortened life expectancy, some modern studies suggest that BMI in the overweight (25-29.9) to class 1 obesity (30-34.9) range does not raise risk for early death.
The potentially lower risk of death in modern studies for people with higher body weight might be explained by improved treatment of conditions such as high cholesterol and blood pressure, common contributors to shortened life expectancy for people with a BMI over 30.
Using BMI to guide recommendations for weight loss
Clinicians commonly use BMI as the metric to decide whether to recommend weight loss, drawing from recommendations such as those released by the United States Preventive Services Task Force, an independent, national panel of health care experts that writes guidelines on preventive health. The task force recommends lifestyle-based weight loss programs such as diet and exercise for adults with a BMI above 30, or above 25 if they have other obesity-associated health conditions such as high blood pressure or high blood sugar. Its members cite the potential for lifestyle-based weight loss interventions to reduce obesity-related health risks as justification for the recommendation.
However, in their 2018 evidence review for these guidelines, task force researchers found no significant improvements in cardiovascular events, mortality or health-related quality of life in studies comparing those who received a lifestyle-based or medication-based weight loss intervention, or both, versus those who did not.
The only specific health outcome that was prevented was developing diabetes. Whether newer, more effective weight loss medications, such as Ozempic, will lead to long-term health benefits remains to be seen.
Part of the reason that the evidence for health benefits of weight loss interventions is so poor is that body weight is regulated by a complicated hormonal system. An adult trying to lose weight with diet and exercise will face indefinite increases in hunger and reductions in daily calories burned as the body attempts to correct weight back to baseline. As a result, even in the optimal setting of clinical trials, the task force found that only 1 in 8 adults would sustain clinically meaningful weight loss of at least 5% of their prior body weight.
Alternatives for assessing weight and health
With the shift away from BMI, the AMA recommends alternative measures that clinicians can use for the assessment of the health risks of an elevated body weight. A variety of measures are suggested, including body adiposity index, relative fat mass, waist-to-hip ratio and waist circumference.
These measures attempt to better characterize fat distribution in the body, given the increased health risks of fat stored around the internal organs. They require additional measurements in a clinic visit. Given the prevalence of anti-fat bias in health care settings, patients may find such measurements to be stigmatizing. Further, while these measurements may better predict health risks of elevated weight, evidence for using these measurements to improve health outcomes is lacking.
In acknowledging the limitations in using BMI as a general measure of health or as a tool to assess the need for obesity treatment, the AMA has taken an important step toward diminishing the role of BMI in clinical practice. Further research is needed to identify the best ways to assess the health risks of elevated body weight.
Scott Hagan, Assistant Professor of Medicine, School of Medicine, University of Washington
This article is republished from The Conversation under a Creative Commons license.
Read the original article.


