ctDNA May Guide Who Needs Chemo After Colorectal Cancer Surgery
February 28, 2024, by Sharon Reynolds
After surgery for colorectal cancer that’s started to spread beyond its initial location, many people go straight to treatment with chemotherapy. The idea behind this postsurgery, or adjuvant, treatment is to reduce the likelihood that the cancer will come back in other places in the body, resulting in more people being cured of the cancer.
But there hasn’t been a method to predict who really needs this extra treatment and who could safely skip it—and avoid any associated side effects.
Results from a new study suggest that there may now be a promising way to identify who does and doesn’t need postsurgical chemotherapy.
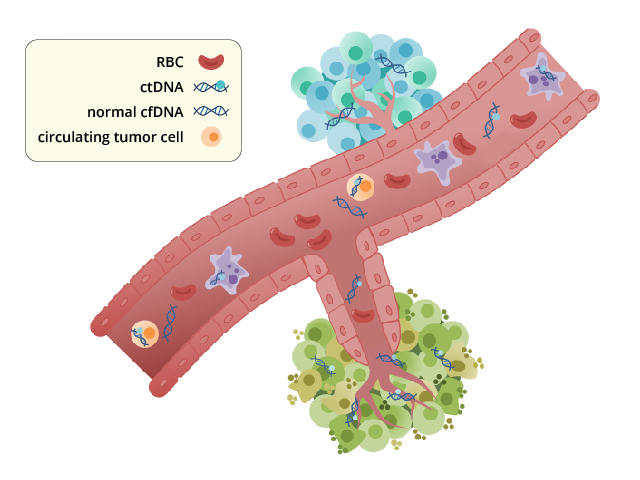
In the study, the presence of fragments of genetic material that have escaped from tumors into the bloodstream, or circulating tumor DNA (ctDNA), seemed to predict which patients would benefit from the chemotherapy they receivedExit Disclaimer. That is, among patients who were ctDNA-positive, those who got chemotherapy lived longer without their cancer coming back (a recurrence) than those who didn’t get chemotherapy.
And, importantly, a negative ctDNA test picked out people who likely hadn’t needed chemotherapy immediately after surgery—in other words, there was no evidence that chemotherapy helped them live longer without a recurrence.
Findings from the study, called BESPOKE CRC and funded by Natera, Inc., which makes the ctDNA test it used, were presented January 20 at the ASCO Gastrointestinal Cancers Symposium. Results from another study using the same test, presented at the symposium by a research team from Japan, showed similar capabilities for ctDNA testing inExit Disclaimer colorectal cancer.
The ctDNA measurements taken in the study, captured with a test called a liquid biopsy, weren’t used to initially choose treatment for individual patients. However, results of the liquid biopsies were provided back to participants and their care teams, to see if those results would change previously decided treatment plans, explained Pashtoon Murtaza Kasi, M.D., M.S., of Weill Cornell Medicine, one of the study’s lead investigators.
But the findings from BESPOKE and the Japanese study are strong enough, he said, to provide assurance that ongoing clinical trials testing ctDNA-driven decisions about whether to use adjuvant chemotherapy are safe and very reasonable to pursue.
“We know that about 60% of people [with this type of colorectal cancer] are cured by surgery,” said Carmen Allegra, M.D., special advisor on gastrointestinal cancer therapeutics in NCI’s Division of Cancer Treatment and Diagnosis, who was not involved with the study. “And we don’t want to expose those patients to chemotherapy and its side effects if we don’t have to.”
But ctDNA may also help identify people who would benefit from even more aggressive treatment after surgery, or who may want to join clinical trials of experimental therapies, said Dr. Kasi.
Two ctDNA tests are already being marketed for monitoring colorectal cancer recurrence and are being used in some clinics. “The problem is, we don’t really know how to use them yet,” said Dr. Allegra.
Currently, if a patient has a positive ctDNA test but imaging tests show no signs that their cancer has come back, there’s uncertainty about whether to start additional treatment right away, he explained.
The ongoing trials will hopefully provide the guidance needed to understand how to best use ctDNA test results to guide patient care, he added.
Tracking a signature of hidden cancer cells
The idea of liquid biopsies that measure ctDNA isn’t a new one. The technology is being widely tested to monitor people with cancer and to potentially detect some cancers early, before symptoms develop.
In terms of guiding treatment, there are two potential uses for such technology: as prognostic tests and as predictive tests. Tests that are prognostic can measure how likely a cancer is to recur after treatment. Tests that are predictive can help inform whether a specific treatment will be effective against an individual’s cancer.
Together, these two types of information could potentially be used to better tailor treatment for colorectal cancer. Researchers have hoped that ctDNA testing could fill these roles, but its actual prognostic and predictive capabilities had remained open questions.
Beginning in 2020, researchers led by Dr. Kasi enrolled almost 1,800 people into the BESPOKE CRC study. The results from their first 623 participants were presented at the 2024 ASCO symposium.
All BESPOKE participants had stage II or stage III colorectal cancer. Cancer at these stages has spread into or through the wall of the colon or rectum and, in some cases, to nearby lymph nodes, but not to distant sites in the body.
The study was not a clinical trial that randomly assigned participants to different groups. All participants underwent surgery and, if decided on by their care team, chemotherapy.
In addition to standard monitoring for cancer recurrence, which includes imaging and blood tests for a protein called CEA, study participants underwent ctDNA testing 1 month after surgery, every 3 months for the next year, then every 6 months for the duration of the study or until their cancer recurred.
A clear difference in benefit from chemotherapy
Of the 623 study participants, 381 received chemotherapy starting about 3 months after surgery, based on how abnormal the cancer cells removed during surgery looked under a microscope and other risk factors.
Of the participants who received chemotherapy, 85 had at least one positive ctDNA test. The other 296 patients who received chemotherapy had negative ctDNA tests.
For people with a positive ctDNA test, chemotherapy provided an obvious benefit. Those patients lived for a median of almost 18 months without their disease returning (a measurement called disease-free survival) compared with about 7 months for people with positive ctDNA tests who didn’t get adjuvant chemotherapy.
But for people with negative ctDNA tests, chemotherapy didn’t make much of a difference. More than 90% of people without measurable ctDNA lived for a median of over 2 years without their disease returning, regardless of whether they received chemotherapy after surgery.
Of the more than 500 participants whose initial ctDNA tests were negative, 14 eventually had a positive test result. These patients were more likely to have their disease recur than patients whose tests remained negative. By 15 months after surgery, however, the likelihood of a patient going from ctDNA-negative to ctDNA-positive dropped sharply.
Out of the 101 patients whose cancer eventually recurred in other organs during follow-up, 40 had what is called oligometastatic disease. This is where a patient has only a few, usually small metastases. A substantial number of these tumors were first picked up by ctDNA testing during the study, Dr. Kasi explained.
For some people with oligometastatic disease, treatment options like surgery or radiation to the sites of metastases are still an option, he continued. “And we know from prior experience that [such treatment] does help improve survival. So ctDNA [testing] may help increase the number of people who may benefit from such an approach.”
How Do Patients Feel About ctDNA Testing?
As part of BESPOKE CRC, the research team also asked patients about how ctDNA testing impacted their mental health—whether it provided peace of mind or more stress.
Overall, participants reported satisfaction with the testing. Scores on tests of anxiety and depression didn’t differ between people whose tests were negative or positive. Almost three-quarters stated that the testing reduced their anxiety about cancer recurrence. And more than 90% said they wanted to continue ctDNA testing to monitor for recurrence going forward.
“I think it’s about an informed patient having more confidence in [the treatment] they are getting, even if [the test isn’t providing] an answer that they wanted to receive,” said Dr. Kasi.
Can ctDNA testing guide treatment from the start?
Studies are now underway to test whether ctDNA measurements can be used to guide colorectal cancer treatment from the outset.
In one of these studies for people with early-stage colon cancer, which is being conducted in the NCI-funded National Clinical Trials Network, people who have a positive ctDNA test after surgery will be randomly assigned to receive a standard chemotherapy regimen or a chemotherapy regimen that is more intensive than usual. “Because it’s very likely these people’s cancer is going to recur,” explained Dr. Allegra.
In contrast, people in the trial with a negative ctDNA test will be randomly assigned to receive only surveillance after surgery or standard chemotherapy. The results from that part of the study will hopefully provide more clarity on who can safely skip adjuvant chemotherapy, Dr. Allegra added.
The BESPOKE results provide assurance that such trials are safe, Dr. Kasi explained.
“When this study was designed several years ago, at that time, to even consider using ctDNA to guide adjuvant chemotherapy was … fraught with a lot of polarized opinions. These results set the stage for ongoing clinical trials,” he said.
For now, the BESPOKE researchers will continue to follow their participants to see if doctors used ctDNA testing information to change treatment strategies in real time, and whether that impacted the risk of cancer recurrence.
Highlighting the need for better treatments
One elephant in the room, said Dr. Allegra, is that around a quarter of patients with stage II or III colorectal cancer won’t be cured even with adjuvant chemotherapy. For someone who has undergone all the standard therapies and still has ctDNA in their blood, “what do you do for that patient?” he asked.
Clinical trials are currently looking at ways to improve outcomes in this scenario, including using different chemotherapy drugs, giving second-line chemotherapy earlier, and testing immunotherapies for tumors with certain genetic characteristics, Dr. Allegra explained.
But results from the patient-reported outcomes from BESPOKE suggest that people want to know what’s happening in their bodies as soon as possible, even if the ctDNA test result is bad news, said Dr. Kasi. And they want to make shared decisions about their future care, he added.
“This test [provides] powerful insights about [whether] to consider [the] next treatment or clinical trial options earlier,” said Dr. Kasi. “It’s also picking up [recurrent] cancer 6 to 9 months before the scans pick it up. I would consider this an integral tool in our toolbox, and it’s here to stay,” he said.
ctDNA May Guide Who Needs Chemo After Colorectal Cancer Surgery was originally published by the National Cancer Institute.