For decades, MENA people in the United States have been classified by the government as ‘white.’
By Nada Hassanein
Stateline
Before the successful, healthy birth of her son, recalls Germine Awad — an Egyptian American who is a psychologist at the University of Michigan — clinicians told her that her hormone levels were too high and that her pregnancy was in danger. “They don’t know us,” her mother reassured her.
Iyman Hamad, a Palestinian American public health graduate student at Wayne State University in Detroit, had to search online to figure out which race or ethnicity box she should check at the doctor’s office and on school forms.
And Itedal Shalabi, who runs an Arab American family services center in the Chicago area and is also Palestinian, said misinformation and hesitancy about COVID-19 vaccines were rampant in her community. Because Arab Americans were considered to be white in the absence of a category for them, county funding for outreach in minority communities was delayed, probably causing avoidable deaths, she said.
“In that time, we had so many Arab Americans die, especially elderly,” she said. “By the time we got the funding, we had so much work to do to catch up, while other [minority] communities were taking advantage of the shot.”
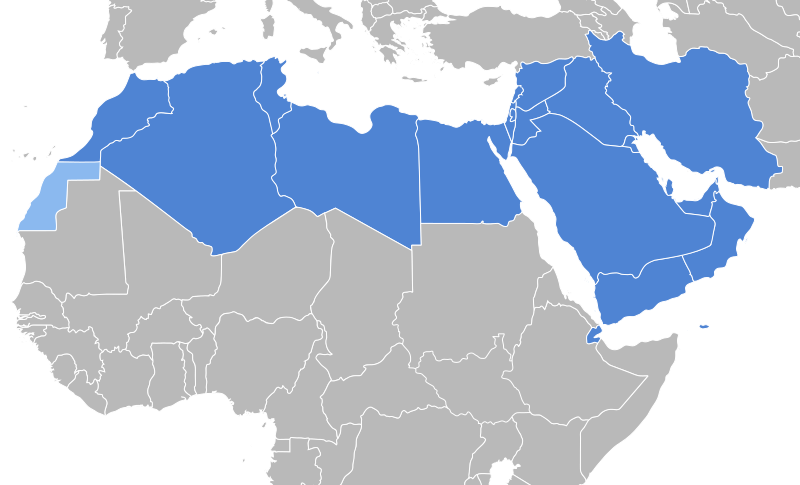
For decades, U.S. residents with heritage from the Middle East and North Africa, which is known internationally as the MENA region, have been classified by the government as white. The grouping masked differences in income, health, housing and other important markers. And when public health officials lack data on COVID-19 deaths or vaccine uptake in the MENA community, for example, it’s difficult to distribute dollars and other public resources effectively.
“The lack of a dedicated identifier makes it hard to isolate data,” said epidemiologist Nadia Abuelezam, an associate professor at the Boston College Connell School of Nursing and the daughter of Palestinian refugees. “Systemically, structurally, we were ignored, or our needs were ignored.”
Last month, the federal Office of Management and Budget approved revisions to race and ethnicity data collection across federal agencies, including the addition of a new MENA category to the census. They are the first race and ethnic category changes since 1997. Along with a combined race/ethnicity category, the changes include a combined Hispanic or Latino checkbox and removal of phrases that can be considered pejorative, including “Negro” and “Far East.” Federal officials have said these revisions will yield more accurate counts and use language “respectful of how people refer to themselves.”
The new federal classification of MENA people is geographical and includes people from Arabic-speaking groups, such as Lebanese, Algerians, Egyptians, Palestinians and Syrians, as well as people from non-Arabic-speaking groups, such as Iranians and Israelis. It also includes ethnic groups who live in multiple countries, such as Assyrian, Kurdish and Chaldean people.
The updates will appear on the next census in 2030, but by next year, federal agencies must submit detailed plans on how they will incorporate the new requirements.
Apart from independent studies by academic and nonprofit researchers, little is known about the health of Middle Eastern and North African people in the U.S. Experts and advocates hope the census change will spur local and state health agencies to update their own data collection methods to shed light on health inequities and needs.
“There’s so many of us here, yet we know so little,” said Hamad, who interns at the Oakland County, Michigan, health department’s data division. “There needs to be change.”
Filling in gaps
Abuelezam, who studies maternal and infant health outcomes among MENA people in Massachusetts, is among a handful of researchers in the U.S. who are trying to fill in gaps in MENA health data.
Her research on Massachusetts mothers has found, for example, that Black Arab mothers had higher odds of preterm birth and low birthweight than Arab mothers classified as white, while Arab mothers were more likely to suffer gestational diabetes than white mothers.
One study found that from the beginning of the pandemic through July 2021, about 17% of Arab Americans in Michigan tested positive for COVID-19 compared with 11% of Hispanic people, 9.8% of Black people and 7.5% of white people.
Similarly, researchers who study aging and Alzheimer’s and related dementias found that confusion and memory issues, which can be early symptoms of the diseases, were found among 17% of MENA immigrants, compared with 9.6% of U.S.-born white people.
The change in categories only applies to federal agencies, not state governments, said Rima Meroudeh, director of the National Network for Arab American Communities. However, the official forms used by states, health agencies and school systems typically mirror the categories used by the census, and the change provides “something much more concrete as we advocate at the state level because they want interoperability between state and federal data,” she said.
Awad, the University of Michigan psychologist, studies mental health and the influence of discrimination in the MENA community. She said the change will help her illuminate social determinants of health, such as housing and environment, income, access to resources, health care and transportation, as well as trauma experiences. Awad and other researchers also are interested in exploring the prevalence of health conditions such as asthma and cardiovascular disease in MENA communities.
“A group of us have been working for years advocating for this box,” Awad said. It’s “been long overdue, and finally, we are going to be able to collect data to truly delve into some unanswered questions. We know there are disparities, but we don’t actually truly understand the extent because there hasn’t been systematic data collection.”
The health data that schools collect also is skewed, said Matt Jaber Stiffler, who co-founded the Center for Arab Narratives, part of the Arab Community Center for Economic and Social Services, or ACCESS. For example, Stiffler said, Arab children are the majority of K-12 students in Dearborn, Michigan, but state data identifies them as white.
Inclusion would “give a better picture of who these communities are and what their needs might be,” Stiffler said.
Population counts
So far, federal population counts of MENA communities have been estimates. For the first time, the 2020 census offered a write-in option so respondents could mark their race and ethnicity as “white” but write in their ancestry. About 3.5 million people wrote in MENA countries of origin, with Lebanese, Iranians and Egyptians making up nearly half of them.
California, Michigan and New York had the largest MENA populations, with more than 300,000 residents combined. Those states were trailed by Texas, Florida, Illinois and New Jersey. Prior to the 2020 write-ins, the American Community Survey, an ongoing survey by the U.S. Census Bureau, provided limited estimates.
According to the Migration Policy Institute, a think tank that analyzes immigration policy, the 1920 census reported around 50,000 people from the MENA region. In the years since, a steady flow of Palestinians, Egyptians, Iraqis, Syrians and others have immigrated to the U.S., some after the 1948 Arab-Israeli War, and many more after the U.S. loosened its restrictive immigration policies in 1965. By 1980, the MENA population in the U.S. had risen to about 224,000.
Last August, Illinois became the first state to enact a law mandating all state agencies that collect race and ethnicity data include a MENA category. Lawmakers in California and Michigan are considering similar bills.
“We should incorporate this at all levels, whether in our health system data or educational systems, like on university levels,” said Sarah Abboud, an assistant professor at the University of Illinois Chicago who studies health outcomes among Arab immigrants.
Some critics argue that the census should move away from categorizing people by race, instead of adding new racial categories. They point to the Human Genome Project, which found that humans share 99.9% of their DNA. Race, some argue, is a social construct, a relic of the 18th century.
But public health experts have demonstrated that racism affects people’s health, and Abboud said that Arab Americans experience worse health outcomes because of it. Additionally, immigrants displaced by war, such as Palestinian and Syrian refugees and their children, may have unique stressors around trauma.
Shalabi, of Arab American Family Services in Chicago, said inclusion of MENA in data is long overdue.
“We’re so excited because it’s about time that our community was identified, was visible, and in a way that really works toward their betterment of health and … being part of the American fabric,” she said.
Originally published by Stateline.
Creative Commons license CC BY-NC-ND 4.0.